.png)
In 2026, a familiar but uncomfortable reality is taking hold for U.S. hospitals.
More organizations will see Medicare payments reduced. Not because of new quality mandates, but because the cumulative impact of readmissions is becoming harder to outrun. Preliminary CMS data for FY 2026 shows that 240 hospitals will face readmission penalties of at least 1%, up from 208 the year before. Nearly 70% of hospitals will still be penalized, even if at lower levels. Very few will escape unscathed.
For many health system leaders, this creates a familiar tension. Readmissions are rarely driven by what happens inside the hospital walls. They're shaped by what happens or rather fails to happen, after discharge: stalled medication titration, missed follow-ups, escalating symptoms, and specialty care that remains episodic rather than continuous.
The result: hospitals are being held accountable for longitudinal outcomes, while much of specialty care delivery is still organized around visits, capacity constraints, and fragmented follow-through. Financial penalties are simply the visible symptom of a deeper structural issue.
It's within this reality that CMS introduced the ACCESS model.
ACCESS solves a problem health systems have struggled with for years: reliably scaling outcomes beyond a narrow subset of patients. Outcome-aligned payments reward measurable health improvements such as lower blood pressure, improved A1c, reduced pain, regardless of delivery method. In person, virtual, asynchronous, or through FDA authorized devices. The flexibility is yours. The accountability is non negotiable.
This is a 10-year foundational pathway where outcome-aligned payments are the default for chronic care delivery. Over 500 technology-enabled care organizations have already submitted intent to apply.
The question for your organization is which ACCESS track offers the fastest path to penalty mitigation, the clearest ROI calculation, and the lowest implementation risk given your current operational reality.
The ACCESS Model offers four tracks aligned to distinct chronic disease populations. The right choice depends on where financial exposure is concentrated today, what infrastructure you can realistically deploy within 12 to 18 months, and which clinical leaders will actively support execution.
Each track solves a different problem and introduces a different operational risk. Treating track selection as a policy decision rather than an execution decision is where most organizations go wrong.
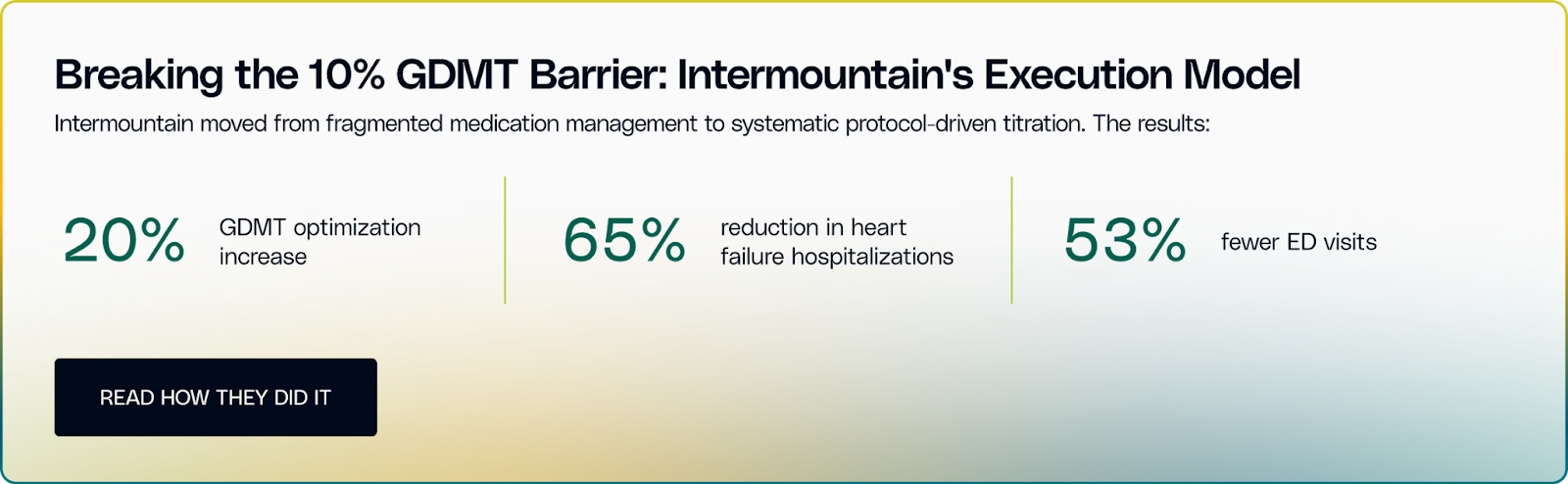
If heart failure readmissions are driving material HRRP penalties, CKM is the most pragmatic entry point. While the track spans diabetes, chronic kidney disease, and atherosclerotic cardiovascular disease, heart failure is where financial exposure is most immediate.
Most organizations already have discharge checklists, follow-up calls, and transition workflows. The breakdown occurs after discharge, when medication optimization and symptom monitoring stall between visits. Fewer than 10% of heart failure patients reach full guideline-directed medical therapy (GDMT) across all four drug classes. Patients begin receiving treatment but the treatment is titrated amidst missed visits, affordability barriers, and overextended cardiology teams.
The real decision is whether your organization can treat medication titration as a continuous operating process rather than a visit-based event. That requires pharmacist- or nurse-led protocols, frequent virtual touchpoints, and remote monitoring reviewed consistently enough to catch early decompensation.
Outcome-aligned payments change the equation. Your pharmacist up-titrates via secure message, your nurse adjusts diuretics from daily weights, your coordinator troubleshoots adherence over the phone. None of these interactions bill under fee-for-service. Under ACCESS, you get paid based on whether patients hit target doses and avoid readmission.
The limiting factor is usually physician acceptance. Protocol-driven titration works only if cardiologists are willing to oversee structured workflows rather than personally manage every adjustment.
✅Choose CKM if readmission penalties represent meaningful financial exposure and your organization is prepared to operationalize continuous medication management outside traditional clinic visits.
While CKM addresses your immediate penalty crisis, it's inherently reactive. You're treating patients who already have advanced disease. What if you could intervene earlier? That's where the eCKM track positions you, though the operational challenges multiply when prevention competes with acute care for resources.
The eCKM track targets hypertension, prediabetes, dyslipidemia, and obesity. Conditions that drive downstream cost, utilization, and chronic disease progression.
Most health systems already see the warning signs: high rates of uncontrolled blood pressure, growing prediabetic populations, and rising obesity. The pipeline for diabetes, heart failure, and chronic kidney disease is already full. The decision to make is: Can we intervene early enough to change patient outcomes?
The operational challenge is that your primary care physicians are already overloaded with chronic disease management, documentation requirements, quality reporting, and referral coordination. Now you're proposing another protocol for hypertension management or lifestyle modification counseling. Without additional support, this fails before it starts.
The real decision is whether you can build prevention infrastructure that operates independently of routine primary care visits. That means care coordinators, health coaches, or dietitians delivering ongoing nutrition, activity, and smoking cessation support between appointments, supported by patient engagement tools that drive accountability without consuming clinician time.
For organizations without internal prevention capabilities, eCKM often requires partnering with technology-enabled care teams that provide virtual coaching, structured programs, and continuous engagement.
The financial tension surfaces quickly. Prevention requires upfront investment with delayed returns. While CKM addresses immediate penalty exposure, eCKM's financial benefit accrues gradually over years through avoided complications and lower utilization.
✅Choose eCKM if your executive team has the patience to invest ahead of downstream risk and your organization can absorb prevention workflows without increasing physician burnout. Deprioritize eCKM if you are in active penalty mitigation mode and lack capacity for delayed-return programs.
The MSK track forces the most explicit trade-off between revenue optimization and population health outcomes. Chronic musculoskeletal pain is commonly managed through procedures that generate near-term revenue but do not reliably improve long-term function or prevent recurrence.
ACCESS shifts MSK care toward conservative, function-first management: physical therapy, behavioral interventions, and longitudinal pain management delivered at scale. Clinically, this approach works. Operationally, it disrupts established referral patterns, procedure volume, and margin assumptions.
The real decision is whether your organization is willing to prioritize functional outcomes over procedural throughput. That is a business model decision that requires board-level alignment and explicit orthopedic stakeholder buy-in.
Execution risk is concentrated in capacity and engagement. In-person therapy is already constrained, and virtual therapy only scales if patients engage and clinicians trust the model. Without investment in scalable therapy infrastructure and change management with orthopedic leadership, MSK underperforms.
✅Choose MSK only if leadership is prepared to manage revenue displacement, align orthopedic incentives, and invest in conservative care pathways that can scale beyond in-person capacity.
The BH track addresses a universal clinical need, but execution is limited by workforce availability and patient engagement. Demand for behavioral health services far exceeds supply, and most health systems lack the licensed clinician capacity required to scale care internally.
ACCESS enables virtual therapy, telepsychiatry, and medication management, but virtual delivery does not solve staffing shortages. Without access to external clinician networks, scale remains constrained regardless of platform capability.
The real decision is whether your organization can secure sustainable behavioral health capacity and integrate it into existing care models. That includes managing regulatory complexity, supporting PCP co-management, and ensuring behavioral health data is incorporated without disrupting clinical workflows.
Patient engagement adds another layer of risk. Acceptance varies by community, influenced by stigma, privacy concerns, and trust in virtual care. Utilization cannot be assumed. It must be understood and actively managed.
✅Choose BH if you already have behavioral health integration underway, are willing to partner for workforce capacity, and have a realistic understanding of how your patient population engages with mental health services. Deprioritize BH if staffing constraints or engagement uncertainty will limit scale.
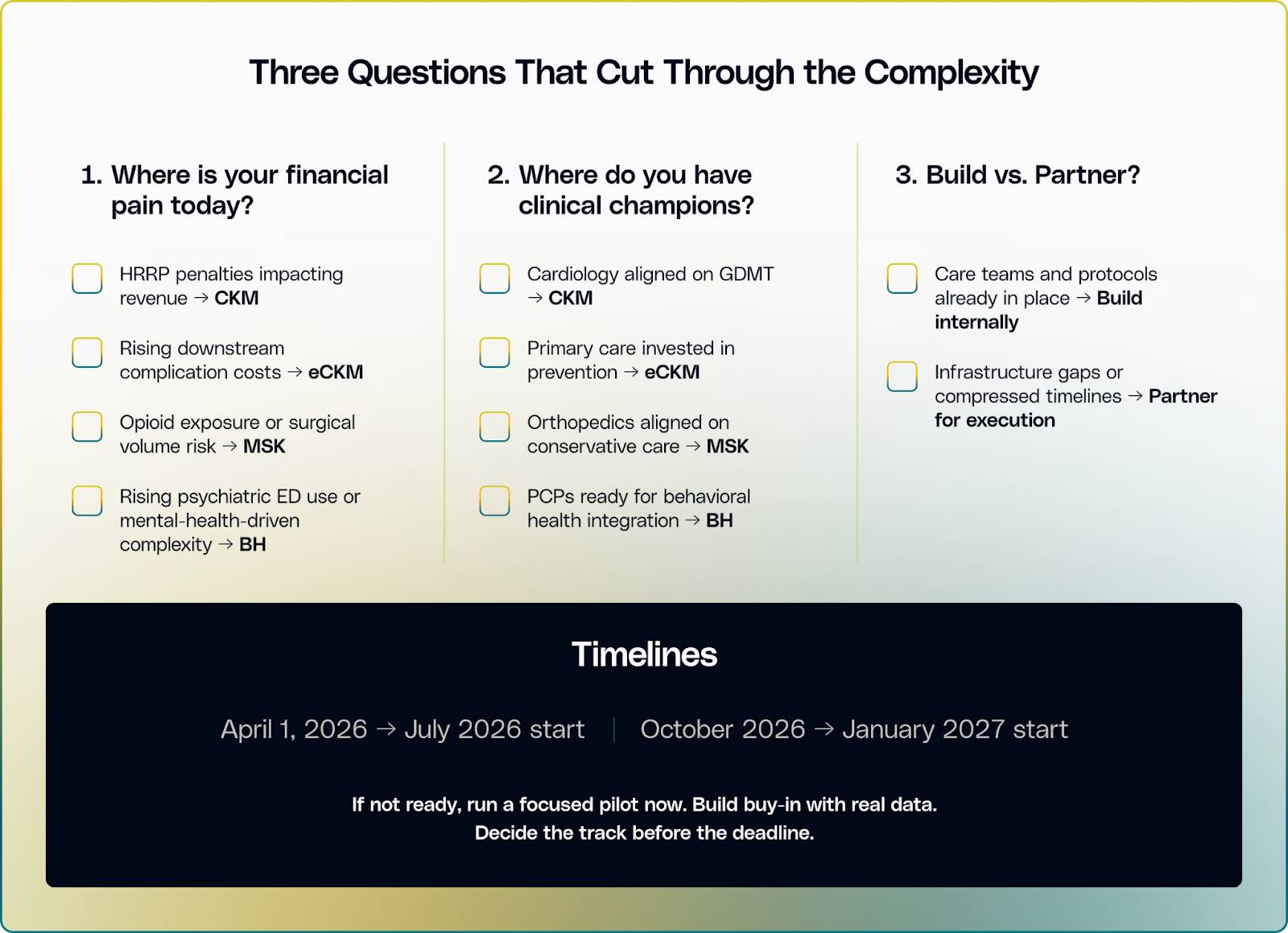
ACCESS represents a permanent shift in how Medicare reimburses chronic care management. For organizations evaluating participation, timing depends on operational readiness.
Building new infrastructure for continuous medication management, remote patient monitoring, and care coordination workflows requires 18 to 24 months under normal circumstances. Most health systems face board approval cycles, budget constraints, and competing priorities that make rapid deployment unrealistic.
For organizations where infrastructure gaps exist, partnership models offer a different execution path. Story Health by Innovaccer provides medication optimization protocols, virtual care team support, and continuous patient engagement systems that integrate with existing EHR workflows: the operational capabilities that enable CKM and eCKM track participation without requiring you to build from scratch or expand internal headcount.
Map your current infrastructure. Assess your organizational timeline. Identify which track aligns with capabilities you can realistically deploy. Make your selection based on execution reality, not aspiration.
If you are determining which ACCESS track fits your patient population and operational readiness, our team can help you evaluate options and define a practical path to participation. Schedule a consultation to continue the conversation.
