"We cannot add staff for this."
That is the boardroom constraint facing rural health systems as they evaluate CMS's Rural Health Transformation Program (RHT).
CMS has committed approximately 50 billion dollars over multiple years to RHT, with funding explicitly directed to evidence-based chronic disease management, technology enabled care, and workforce efficiency in rural communities.
If chronic care in your market is still visit-bound, you will lose patients to systems that can respond between visits. Because deterioration happens on weekdays, weekends, and long drives home, and your current workflows do not reliably "see" it until it becomes utilization.
With workforce constraints across rural counties, it is essential to design sustainable care models that improve outcomes while maximizing available resources. This is where intelligent care orchestration matters. Not as a concept, but as a practical answer to the question RHT introduces: How do you deliver continuous specialty care without changing your entire workflow or hiring a team you cannot recruit?
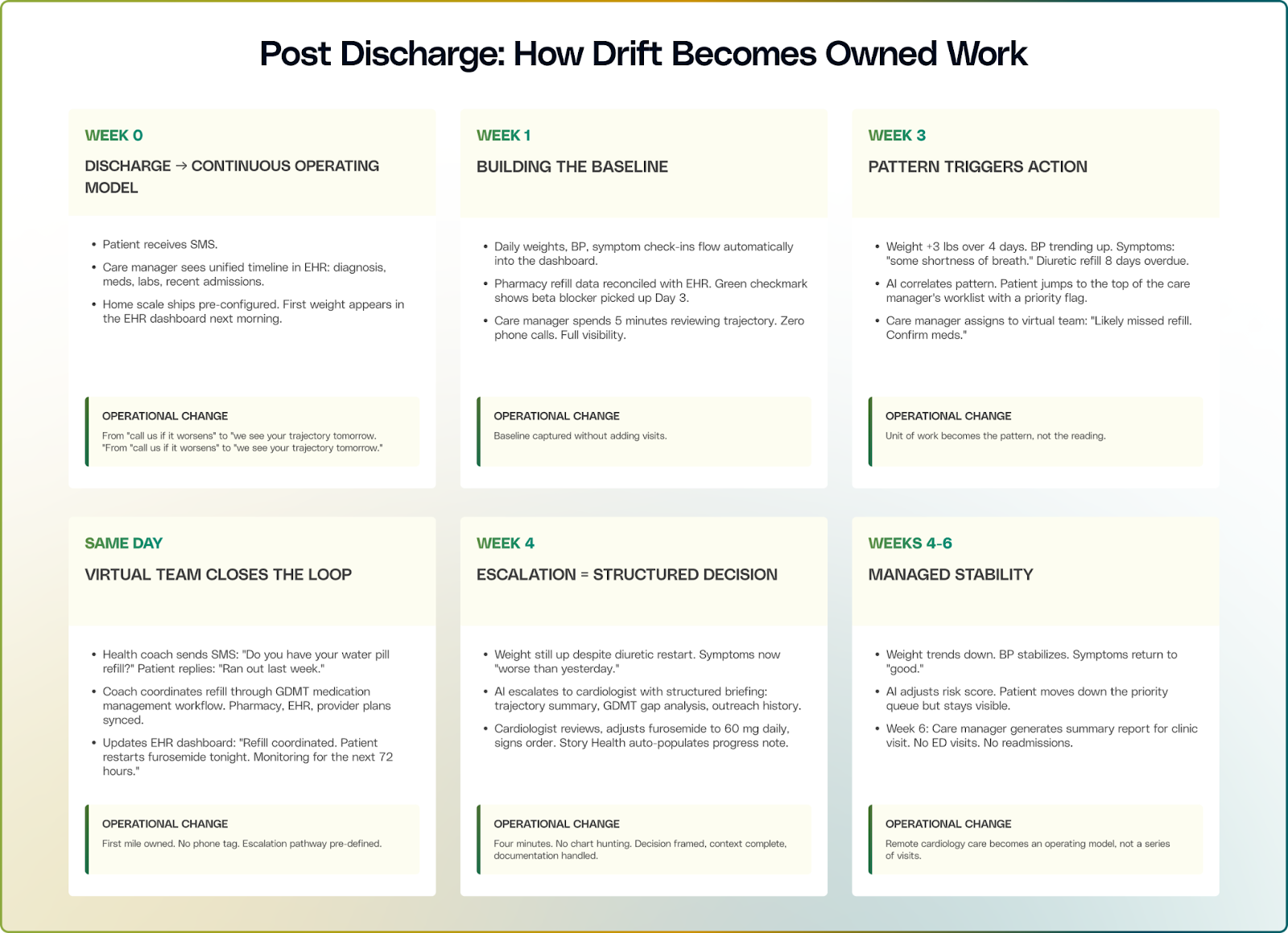
What happens in the first six weeks after discharge is crucial. That is where drift turns into admissions, and where "continuous care" either exists or it does not.
In rural markets, geography makes access harder, but it is not the root problem. The root problem is that early cardiac infarction drift rarely has a clear owner, a clear response time, and a clear playbook.
When those three are not hard-wired, your team defaults to the safest operational behavior: defer anything that is not unmistakably urgent. That is how you end up with a program that is busy, but inconsistently responsive.
RHT exposes that inconsistency, because it requires you to demonstrate sustained improvement, not document activity.
So the question becomes simple: Can you name, in one sentence, who owns "drift" in chronic care, and what happens next?
If you cannot, you are not running a sustainable chronic care model. You are running a data layer that still depends on individual vigilance.
Most cardiology programs already have pieces: an EHR, some home monitoring, a care manager, and clinicians who want GDMT optimized. The problem is how those pieces connect, or don't.
Here is what changes when your healthcare infrastructure works together:
Before: your nurse reconstructs context → After: the system assembles the trajectory
Instead of forcing staff to hunt across portals, notes, and pharmacy workflows, the patient's history is assembled as one longitudinal timeline. That is the only way to make "early drift" visible without adding more staff.
Before: thresholds flatten urgency → After: patterns create priority
A blood pressure spike, a two-pound weight change, and a missed refill can look like three unrelated events. In heart disease, they are often one pattern of early decompensation. Pattern-based triage separates noise from risk and routes work accordingly.
A 2025 meta-analysis of randomized trials found that non-invasive remote patient monitoring was associated with lower mortality risk and reduced first HF hospitalization risk compared to usual care, particularly when programs included education and self-management support alongside monitoring. The evidence is clear: outcomes move when monitoring is embedded in an operational loop that converts signal into action.
Before: escalation is a message → After: escalation is a decision point
Clinicians do not need more alerts. They need a structured task that frames the decision with the relevant trend, medications, and tolerance context so action can happen quickly.
Before: follow-through depends on local bandwidth → After: virtual capacity handles between-visit work
Rural systems lose control in the days between visits. A virtual care team can handle outreach, adherence friction, and patient coaching, then escalate only when clinical judgment is needed.
Those changes sound straightforward. The operational question is what actually assembles the trajectory, prioritizes the patterns, and routes the work.
RHT is pushing rural systems toward sustainable access through coordinated operations and technology. Cardiology is where that intent gets tested first, because it punishes episodic models quickly.
The answer is not more visits. It is constant, connected oversight that protects both your patients and your teams. That does not mean hiring an army. It means an operating system that does three things well:
It keeps a live, unified story of each patient so no one is stitching history together from disconnected information. It uses intelligence to prioritize the right patients every day so you spend scarce time where it changes trajectory. It wraps that intelligence in virtual and local workflows that deliver timely intervention without burning your people out.
This is what your board will expect to see when they ask what RHT dollars produced. A drop in readmissions, a clear story about how you used technology to protect your workforce, and evidence that your system can run continuous chronic care with the staff you have, not the staff you wish you had.
Story Health customers have demonstrated heart failure readmission reductions of 30%, measurable improvements in guideline-directed medical therapy adherence, and sustained declines in emergency department utilization. These results reflect programs where AI-powered orchestration and virtual care delivery operate as one system, expanding clinical capacity without adding headcount.
If you are ready to see what that looks like for your own cardiac care program, book a session with the Story Health team.

